When language becomes a barrier to paediatric clinical trials
A child’s language should not close the door to a clinical trial
For children living with rare or serious diseases, a clinical trial in another European country may be the only opportunity to access an investigational treatment. Yet Europe’s linguistic diversity can turn language into an unspoken border: families may be unable to participate simply because they do not speak the language named in a study protocol.
Our new paper, published in Pharmaceutical Medicine, asks a direct question: how often is language used as an eligibility criterion in paediatric clinical trials in Europe, and when is that restriction scientifically justified?
This work is a very nice collaboration between B2SLab at IRIS | UPC and Begonya Nafria at the Patient Engagement in Research Department, Institut de Recerca Sant Joan de Déu (IRSJD), alongside an international group of experts in paediatric research and cross-border clinical trials. It brings data science, patient engagement, clinical research, and ethics together around a practical question: how can trial design avoid excluding children and families unnecessarily?
What the study examined
The team searched the eligibility criteria of 1,754 phase I-III paediatric clinical trials conducted in Europe between 2007 and 2024 and registered on ClinicalTrials.gov. Using a Python-based workflow, we looked for references to the continent’s 32 official languages, as well as terms connected to language and cross-border participation. Each identified requirement was then manually reviewed in its protocol context.
Not every language requirement is inappropriate. For example, it can be justified when a trial relies on a language or cognitive assessment, or on a patient- or caregiver-reported outcome measure that has been validated only in a particular language. The key question is whether the requirement is necessary for the study’s scientific aims - rather than a convenient stand-in for the resources needed to include a family.
What we found
Most protocols (95.2%) did not explicitly refer to language in their eligibility criteria. However, 85 protocols (4.8%) did. Of those 85, only 23 (27.1%) contained a scientific justification for the language requirement. English and French were the most frequently specified languages.
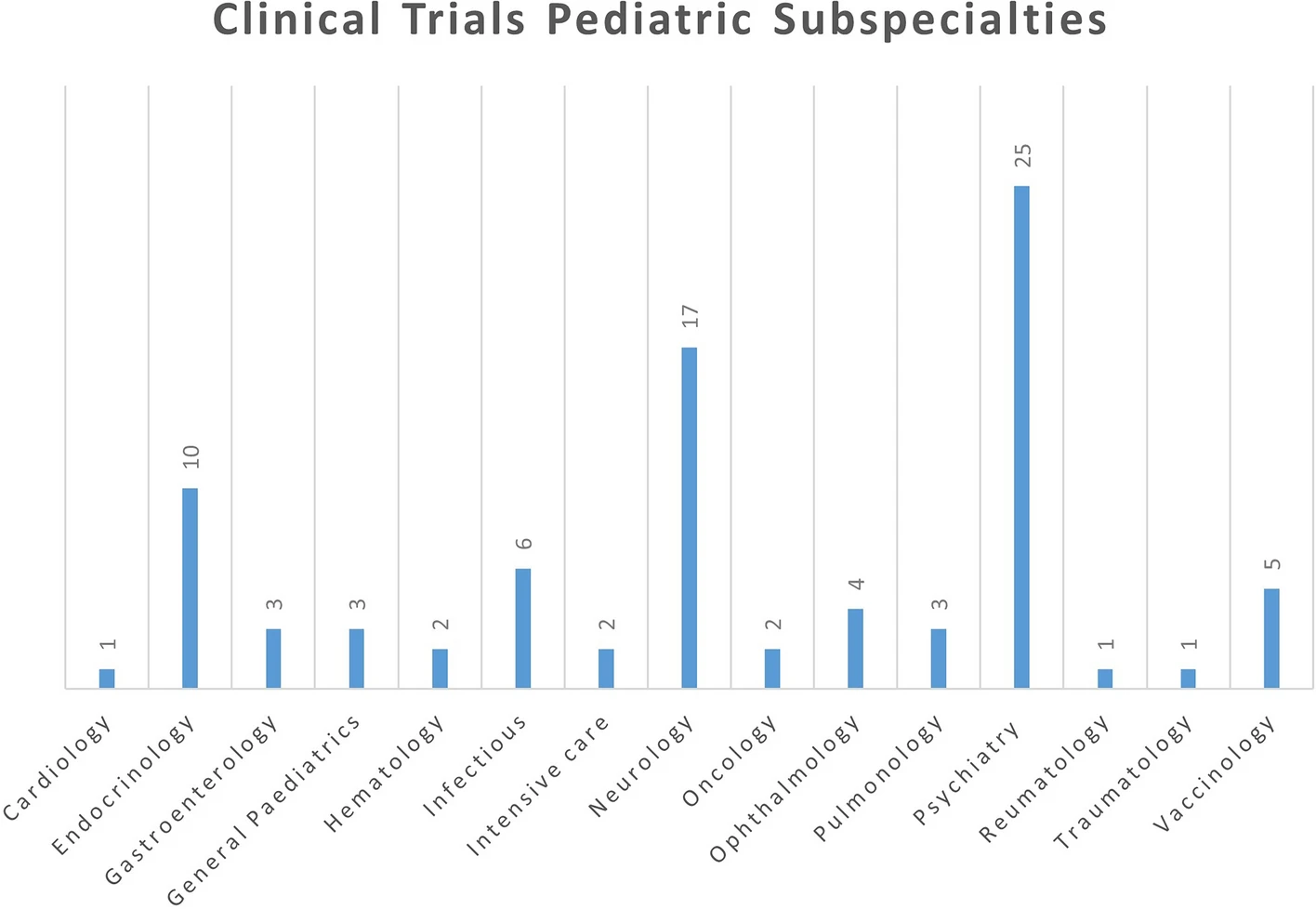
The figure below shows the paediatric subspecialties represented among the protocols that included language-related terms. Psychiatry (25 trials) and neurology (17 trials) were the most frequent, followed by endocrinology (10 trials).
Language restrictions also overlapped with other possible barriers to participation. The review identified requirements related to a particular national healthcare system, travel, phones, or internet access. These practical constraints matter especially for rare diseases, where the appropriate trial may only be available far from a family’s home.
Designing trials that welcome, rather than exclude
The study does not argue that every clinical trial must operate in every language. Instead, it shows why protocols should be explicit when a language criterion is genuinely required - and why ethics committees should ask for that justification. If a barrier is logistical, it may be possible to address it through translated materials, interpreters, remote visits, travel and accommodation support, or satellite sites.
The authors recommend two concrete additions to trial protocols: a dedicated cross-border access section that defines objective criteria and support for international participants, and an inclusive recruitment plan that anticipates the needs of the patient groups a study should represent. Involving young people and caregivers early in protocol development can help identify these barriers before they become reasons for exclusion.
Making paediatric research more inclusive is not simply a matter of fairness. It also helps ensure that trial findings represent the children who may eventually need the treatment.
Reference: Nafria B, Perera A, Gaillard S, et al. Language as an Eligibility Criterion in Pediatric Study Protocols Conducted in Europe (2007-2024) Reported in the ClinicalTrials.gov Database. Pharmaceutical Medicine (2026). https://doi.org/10.1007/s40290-026-00613-1