Is your child’s copper level really normal? Why inflammation makes this question harder than it looks
Copper: essential, but tricky to measure
Copper is an essential trace element. Too little causes anaemia, neurological problems, and immune dysfunction; too much can be toxic. In children — whose copper needs and metabolism change rapidly across development — knowing whether a measured blood level is truly normal or abnormal is clinically important.
The standard approach is to compare a patient’s result against a reference interval: the range of values observed in healthy people of the same age. But establishing reliable reference intervals for children faces two well-known challenges.
First, copper levels change substantially with age. A value that is perfectly normal in a newborn may be elevated in a five-year-old. This means age-stratified or, better, age-continuous reference intervals are needed.
Second — and this is less widely appreciated — inflammation raises copper. When the body mounts an inflammatory response, it increases production of ceruloplasmin, the main copper-carrying protein in blood, which drives up measured copper levels. A child with an ongoing infection or chronic inflammatory condition may appear copper-replete on paper while actually being at risk.
A large paediatric dataset and a new model
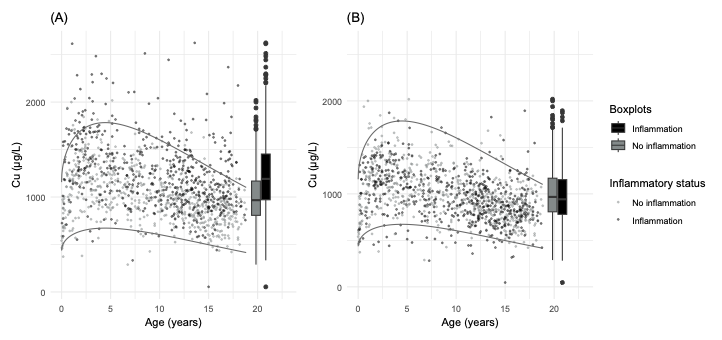
In a new study published in Clinical Nutrition, our team — in collaboration with Hospital Sant Joan de Déu Barcelona — analysed 4,368 paediatric serum samples to build a more accurate framework for interpreting copper measurements in children.
Using the same continuous reference interval methodology we developed for cerebrospinal fluid amino acids and neurotransmitter metabolites, we modelled copper concentration as a function of age using nonlinear regression, then assessed the contribution of inflammatory markers — specifically erythrocyte sedimentation rate (ESR), fibrinogen, and C-reactive protein (CRP) — to residual variability.
The results were clear: inflammation elevated measured copper by approximately 24% on average. Children with active inflammation would therefore appear to have higher copper than they truly do after accounting for their biological state. Using uncorrected reference intervals in such patients risks under-diagnosing copper deficiency.
The solution: an inflammation-adjusted score
To address this, we built a composite inflammation score using partial least squares regression across the three inflammatory markers. This score captures the combined inflammatory load of a patient and allows copper measurements to be adjusted accordingly before comparing them against the reference interval.
The result is a proof-of-concept model that produces age- and inflammation-adjusted reference intervals — the first of their kind for paediatric serum copper.
Practical impact
For clinicians managing children with suspected metabolic disorders, chronic diseases, or nutritional deficiencies, this work offers a more reliable interpretive tool. It also extends our group’s broader programme of establishing statistically robust, age-continuous reference intervals for paediatric laboratory biomarkers — a methodology we have previously applied to cerebrospinal fluid amino acids and biogenic amines.
The paper is available at: Rodriguez-Gonzalez H, Arias A, Poyatos E, et al. Proof of concept for an age- and inflammation-adjusted model for the establishment of pediatric serum copper reference intervals. Clinical Nutrition, 2026. https://doi.org/10.1016/j.clnu.2026.106586